The Effectiveness of Continuous Passive Motion (CPM) in Knee Rehabilitation: A Comprehensive Review
Continuous Passive Motion (CPM) has been a widely used rehabilitation technique for patients recovering from knee surgeries, particularly total knee replacement (TKR). However, recent research has raised questions about its effectiveness compared to other rehabilitation methods. This blog post will explore the current evidence surrounding CPM and its impact on knee rehabilitation outcomes.
Understanding Continuous Passive Motion
CPM is a rehabilitation technique that uses a motorized device to move a joint passively through a controlled range of motion. The primary goal of CPM is to promote healing, reduce joint stiffness, and improve range of motion (ROM) following surgery or injury.
Research Findings on CPM Effectiveness
Range of Motion Improvements
Several studies have investigated the impact of CPM on knee range of motion:
- Meta-analysis by Wu et al. (2008): Found that CPM use led to a 5° greater total Range of Motion (ROM) compared to physical therapy alone.
- Zhengfeng Jia et al. (2024): Indicated that CPM increased active knee flexion ROM by only 2 degrees (95% CI 0 to 5) or an absolute improvement of 2% (95% CI 0% to 4%).
- Meta-analysis of nine studies: Concluded that CPM had no significant effects on active knee flexion and active knee extension compared to non-CPM therapy.
These conflicting results suggest that while CPM may provide some improvement in ROM, the gains are generally small and may not be clinically significant.
Actual vs. Programmed Motion
An important consideration when evaluating CPM effectiveness is the discrepancy between programmed and actual knee motion. Research by Maniar et al. (2012) revealed that the knee experienced only 68% to 76% of the programmed CPM arc. This finding suggests that the actual benefits of CPM may be even less than initially thought.
Comparison with Other Rehabilitation Methods
- Meta-analysis of nine RCTs (up to 2014): Found no significant difference in ROM and knee extension between patients treated with CPM and those who were not.
- Systematic review by Zhengfeng Jia et al. (2024): Involving 557 patients, showed similar outcomes in passive knee flexion and extension between CPM and physical therapy. CPM was also associated with higher costs and longer hospital stays.
These findings suggest that CPM may not offer significant advantages over traditional physical therapy techniques.
Limitations of CPM
Passive Nature of the Treatment
One of the main limitations of CPM is its passive nature. While it aims to improve joint flexibility through passive movement, it often fails to significantly enhance ROM or patient satisfaction when compared to more active rehabilitation methods. Passive movement lacks the intensity needed to break down scar tissue effectively.
Treatment Duration and Patient Engagement
CPM treatment sessions can vary widely, from as little as 1.5 hours to as much as 24 hours per day for arthrofibrosis cases. This wide range in treatment duration can lead to inconsistent results and potentially higher treatment costs compared to more dynamic and patient-engaged rehabilitation methods.
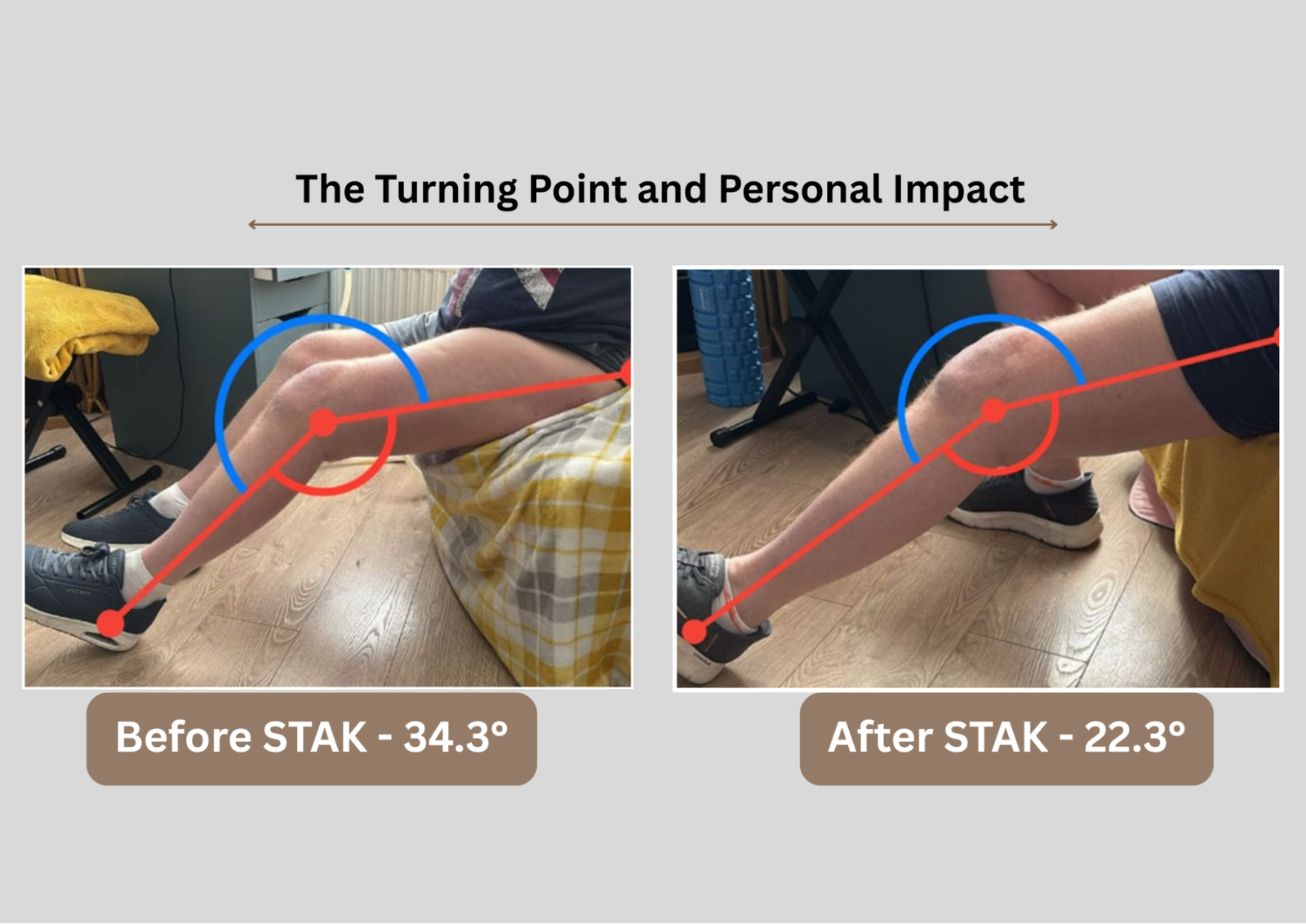
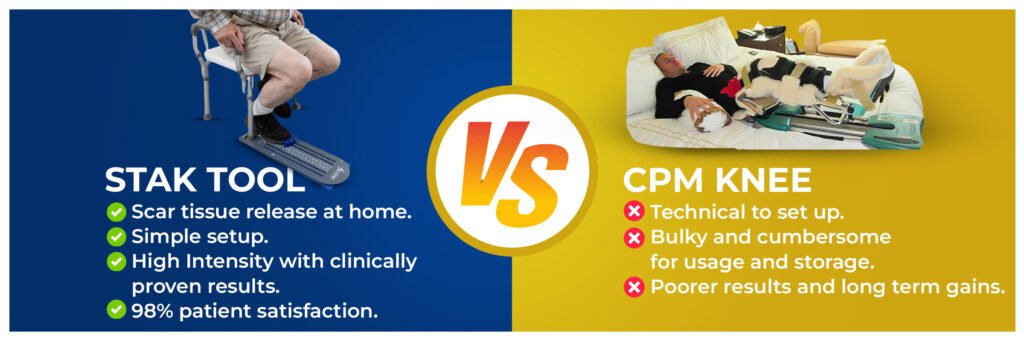
Alternative Approaches: The STAK Tool
In contrast to CPM, newer rehabilitation tools like the STAK tool integrate active, dynamic, and high-intensity stretching techniques that are essential for breaking down scar tissue and promoting joint flexibility.
Advantages of the STAK Tool
- Active Engagement: Facilitates intensive and targeted rehabilitation while enhancing patient engagement and motivation.
- Progress Tracking: The measuring scale enables patients to track their progress step by step, setting and achieving targets to maintain motivation.
- Patient Control: Provides full control over the intensity of the stretch, allowing for a personalized rehabilitation experience.
- Comprehensive Rehabilitation: Includes active assistive range of motion (AAROM) and resistive range of motion techniques, addressing all critical aspects of rehabilitation.
| Feature | STAK Knee Tool | CPM |
|---|---|---|
| Ease of Use | Light and easy to use. | Bulky and complicated to operate. |
| Time commitment | 20 minutes 3 x a day plus warm up, cool down. | Minimum 4 hours – 14 hours a day. |
| Speed of Improvement | Quick, noticeable improvements often within first session.Improved ease of daily activities. | Slow progress, low intensity movement with poor carryover into daily activities. |
| Range of Movement and lasting improvement | Transformation in range of movement in 4-8 weeks.Proven lasting mean 30° in movement. | Slow improvement in range of motion, research shows no lasting gains. |
| Effectiveness and Motivation | Highly effective and motivating. | Often lacks user engagement and motivation,leading to lower compliance. |
| All-round knee rehabilitation tool | Optimise range of movement, strengthen, and function before and after surgery. | Provides no strengthening elements focusing mainly on gentle passive movement. |
| Preparation for Surgery | Prepare for knee replacement surgery with confidence using the STAK programme. | Does not provide specific pre-surgery training or preparation. |
| Post-Surgery Recovery | Enhances mobility and strength preoperatively, promoting smoother recovery and better outcomes post-surgery. | May not significantly improve mobility or strength before surgery, affecting postoperative recovery. |
Implications for Clinical Practice
Key Considerations for Healthcare Providers
- Reassessment of CPM Use: Healthcare providers should carefully consider the use of CPM in knee rehabilitation protocols, given the limited evidence of its effectiveness.
- Focus on Active Rehabilitation: Greater emphasis should be placed on active rehabilitation techniques that engage patients and promote more effective recovery.
- Cost-Effectiveness: Given the higher costs associated with CPM and its limited benefits, healthcare providers should consider more cost-effective alternatives.
- Individualized Treatment Plans: Rehabilitation protocols should be tailored to individual patient needs, considering factors such as the type of surgery, patient age, and overall health status.
Conclusion
While Continuous Passive Motion has been a staple in knee rehabilitation for many years, current research suggests its effectiveness may be limited. The small gains in range of motion, coupled with the discrepancy between programmed and actual knee motion, raise questions about its clinical significance.
Alternative approaches, such as the STAK tool, which incorporate active, dynamic stretching techniques, show promise in improving rehabilitation outcomes. These methods not only address the limitations of CPM but also promote greater patient engagement and potentially more effective recovery.
As the field of knee rehabilitation continues to evolve, healthcare providers must stay informed about the latest research and consider adopting more effective and efficient rehabilitation methods. This approach will help optimize patient outcomes, manage healthcare costs, and ultimately provide better care for individuals recovering from knee surgeries or injuries.
References
- Zhengfeng Jia et al. (2024). Efficacy and safety of continuous passive motion and physical therapy in recovery from knee arthroplasty: a systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research, 19, Article number: 68.
- Maniar RN, et al. (2012). Comparative study on the use of continuous passive motion post-total knee arthroplasty.
- Harvey L.A., Brosseau L., Herbert R.D. (2014). Continuous passive motion following total knee arthroplasty in people with arthritis. Cochrane Database of Systematic Reviews, 2014; 2nd ed.
- Wu J., Lv M., Zhou Y. (2008). Effectiveness of prolonged use of continuous passive motion (CPM) after total knee arthroplasty. Annals of Joint.
- Verywellhealth.com. Continuous Passive Motion (CPM Machine): Uses, Side Effects
- Wu J., Lv M., Zhou Y. Association of knee range of motion and continuous passive motion following total knee arthroplasty: a meta-analysis. Ann Jt. 2016; 1
- Aspinall, S. K., Bamber, Z. A., Hignett, S. M., Godsiff, S. P., Wheeler, P. C., & Fong, D. T. P. (2021). Medical stretching devices are effective in the treatment of knee arthrofibrosis: A systematic review. Journal of orthopaedic translation, 27, 119-131.
- Physio-pedia.com. Continuous Passive Motion (CPM)