Knee osteoarthritis (OA) is becoming increasingly prevalent among the working-age population. The number of total knee replacements (TKRs) performed on individuals under 68 years old has risen significantly, with a 188% increase observed between 2000 and 2015 (AAOS, 2014). This trend is attributed to rising obesity rates, sedentary lifestyles, an ageing workforce, and increased physical demands in certain occupations.
The Impact of Early TKR
While TKR is often an effective treatment for severe knee OA, it presents unique challenges for some younger patients:
1. Approximately 20% of TKR patients report dissatisfaction with the outcome, with younger patients more likely to experience ongoing pain and stiffness (Bourne et al., 2010).
2. The average lifespan of a knee implant is about 15-20 years, potentially less for those in physically demanding jobs (Kurtz et al., 2007).
3. Research indicates that TKR performed under age 55 often leads to poorer satisfaction and outcomes (Parvizi et al., 2014).
These factors underscore the importance of delaying surgery when possible and exploring alternative management strategies.
Preventive Strategies and Early Intervention
Occupational health professionals play a crucial role in helping employees manage knee OA and potentially delay the need for surgery. Here are some key areas to focus on:
The Value of Pre-habilitation
Pre-habilitation, or “prehab,” has gained recognition for its potential to improve outcomes both before and after surgery. Implementing strength training, flexibility exercises, and cardiovascular conditioning can help patients better prepare for surgery or potentially delay its necessity.
Weight Management and Exercise
Excess weight puts additional stress on knee joints. Every pound of weight gained results in an additional four pounds of pressure on the knees . Encouraging weight loss through diet and exercise can significantly reduce knee pain and slow OA progression. For patients who find weight-bearing exercises painful, recommend low-impact alternatives such as:
• Stationary cycling
• Aqua jogging
• Swimming
Every pound of weight gained results in an additional four pounds of pressure on the knees.
Pain and Inflammation Management
Effective pain control is crucial for maintaining mobility and function. Advise patients to:
1. Take prescribed pain medication as directed, maintaining a regular schedule rather than waiting for pain to become severe.
2. Use ice therapy regularly, especially if unable to take anti-inflammatory medications.
3. Consider topical anti-inflammatory gels as an alternative to oral medications.
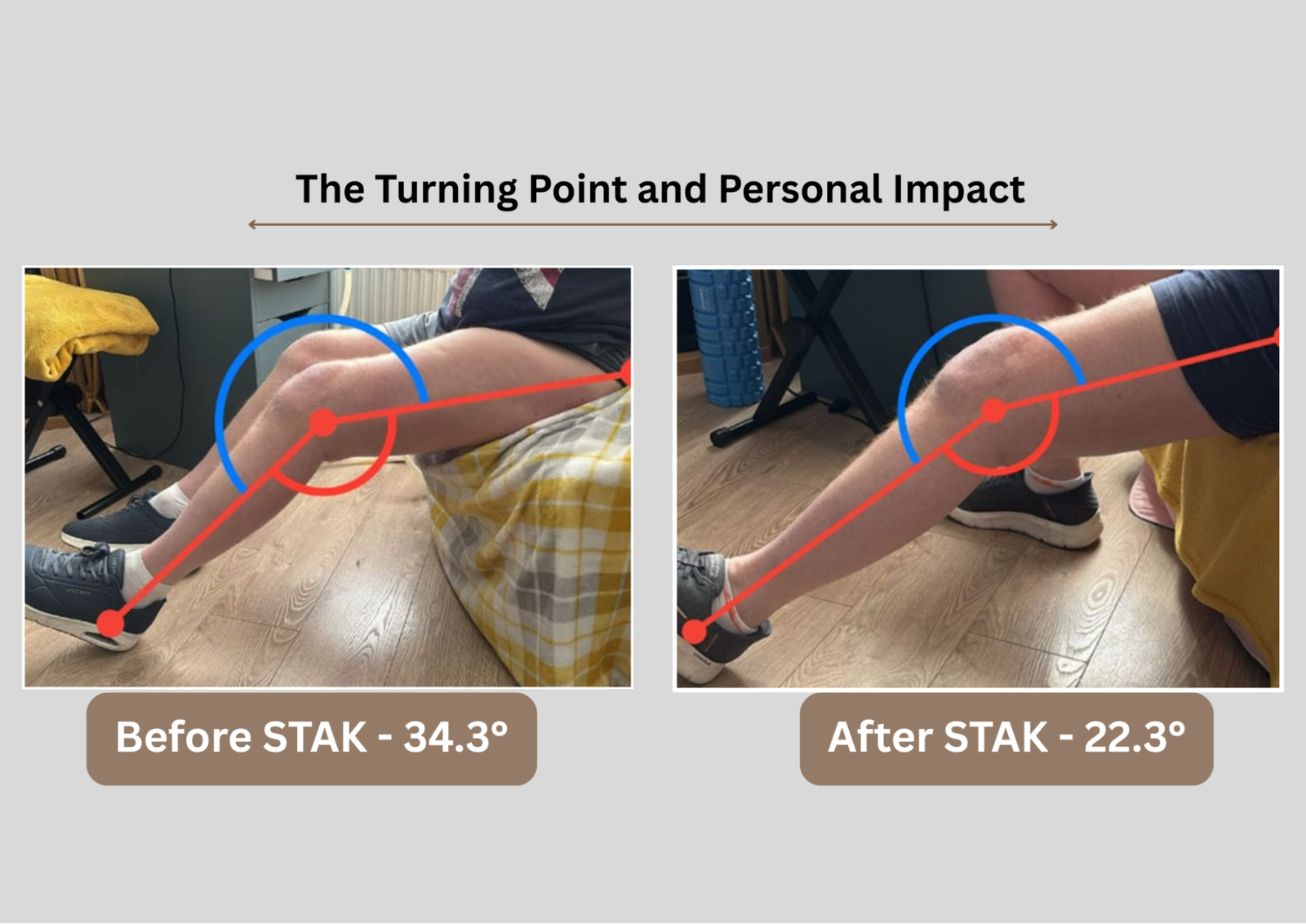
Maintaining Knee Extension
Loss of knee extension (straightening ability) can lead to gait abnormalities and muscle imbalances. Even a small extension deficit of 3° to 5° can affect walking patterns, leading to:
• Increased quadriceps activation
• Calf muscle tightness
• Altered patellofemoral mechanics
• Reduced gluteal muscle activity
Research indicates that limited knee extension during gait can cause abnormal joint loading and increased strain on the patella tendon, which in turn affects the overall gait pattern and muscle function (Shelbourne and Gray, 1997).Early identification and treatment of extension deficits are crucial. Recommend exercises such as hamstring stretches, calf stretches, and quadriceps exercises.
Key Tips for Patients
1. Education: Provide information on weight loss, diet, and appropriate cardiovascular exercises.
2. Pain Control: Encourage regular use of prescribed pain relief as directed.
3. Inflammation Management: Emphasise the importance of ice therapy.
4. Maintain Knee Extension: Teach patients to recognise and address early signs of extension loss.
5. Low-Impact Exercise: Recommend non-weight-bearing exercises like stationary cycling or swimming.
Dr Aspinall’s Top Tips for Managing Knee Osteoarthritis
1. Minimise Inflammation
• Modify activity where possible
• Educate about the importance of pain killers/anti-inflammatories; unpick negative beliefs
• Don’t underestimate the power of ice – encourage icing at work during breaks
Ice knee regularly – 15 – 20 minutes
2. Daily Routine
•Calf stretch: 3 Repetition 30 Seconds
• Seated hamstring stretch: 3 x Repetition hold 30 seconds
• Knee extensions while sitting in a chair to end of range extension: 10 times, hold for 5 seconds
Knee extension- quadricep strengthening exercise
• Gluteal and core activation bridge: 10 times, hold for 5 seconds.

3. Weight Management
• Educate about the power of weight loss in reducing knee stress and pain.
References
1. Arthritis Foundation. “Osteoarthritis of the Knee.” Available at: Arthritis Foundation.
2. AAOS (2014). American Academy of Orthopaedic Surgeons Annual Meeting Proceedings.
3. Bourne, R. B., et al. (2010). “Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not?” Clinical Orthopaedics and Related Research, 468(1), 57-63.
4. Kurtz, S. M., et al. (2007). “Future clinical impact of revision total knee arthroplasty in the United States: a population-based projection.” The Journal of Bone and Joint Surgery, 89(3), 1-8.
5. Parvizi, J., et al. (2014). “High level of residual symptoms in young patients after total knee arthroplasty.” Clinical Orthopaedics and Related Research, 472(1), 133-137.
6. Shelbourne, K. D., & Gray, T. (1997). “Minimum 10-year results after anterior cruciate ligament reconstruction: How the loss of normal knee motion compounds other factors related to the development of osteoarthritis after surgery.” The American Journal of Sports Medicine, 25(5), 591-595.